
Healthcare workers conduct COVID-19 testing on the Navajo Nation in May in Tonalea, Ariz. The Arizona National Guard helped conduct a statewide testing blitz. Photo Sgt. Michael Matkin, 161st Air Refueling Wing Public Affairs
WINDOW ROCK, AZ — The Indian Health Service) and the Native American communities it serves saw the COVID-19 pandemic’s impact reach new heights in May.
The Navajo Nation, which straddles Arizona, New Mexico and Utah, became the new epicenter for the virus in the United States, with 4,000 cases reported out of a population of 173,000 as of mid-May. This surpassed the infection rates in New York and New Jersey.
In a media call on May 14, Loretta Christenson, MD, chief medical officer of the Navajo Area Indian Health Services, said that, while the surge of patients has been difficult for the community and the health service, it had not been unexpected.
“We worked on a surge plan long before this COVID crisis came into fruition,” she explained. “Our predictions did occur pretty much on time with our models, [and] this allowed us to prepare for what would happen in regard to volume of patients. We doubled our ICU volumes and tripled the amount of patients we transferred to tertiary centers.”
While the surge numbers have been extreme, they still did not reach the peaks that IHS’s models had predicted, which Christenson credits to early social distancing efforts.
“We’re doing very well during this time because we had the opportunity to use our tertiary partners in New Mexico and Arizona, where we’ve been able to send our most critical patients,” Christenson explained.
Meanwhile, IHS is close to making an announcement on a contract for acritical care response team, explained IHS Chief Medical Officer Rear Adm. Michael Toedt, MD.
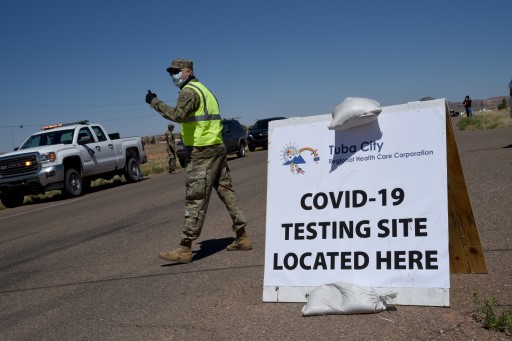
In mid-May, the Arizona National Guard helps with a statewide testing blitz at the Navajo Nation in Tonalea, AZ. Native Americans have been hit especially hard by the COVID-19 pandemic. Air National Guard photo by Tech. Sgt. Michael Matkin).
“The team would deploy when needed to deploy urgent life-sustaining medical care for patients with suspected or confirmed COVID-19,” Toedt explained. It also would train staff at hospitals on best COVID-19 care practices.
Toedt also lauded IHS’s efforts in increasing testing across Native communities. As of May 12, IHS had distributed 250 Abbott ID-NOW rapid analyzer machines and over 90,000 tests across its network, he said.
Since then, however, questions have been raised as to the test’s effectiveness. Study results released in April showed an 85% rate of reliability in recognizing positive samples. Subsequent studies suggest that rate may be lower—something that has raised concerns among tribal leaders.
On May 14, the Food and Drug Administration issued an alert warning the public that the tests may return false negative results. FDA officials noted that, while the test can still be used to correctly identify positive cases in minutes, negative results may need to be confirmed with a high-sensitivity molecular test.
The CARES Act that passed at the end of March provided an estimated $1 billion to the IHS. A little under half of that was designated to IHS-directed health programs, tribal health programs and urban Indian organizations. The rest would be used on telehealth, medical equipment, sanitation and potable water needs, testing kits, and other pandemic-related needs.
The bill also included $8 billion in funding directly to Native nations. However, allocation of that funding was delayed until early May.
When a patient has all or most of the clinical symptoms and signs, in the context of a epidemic, and other processes have been ruled out, a negative test should be viewed with suspicion. With clinical judgement overruling a negative test.
We just had a patient with all the classical symptoms and signs of covid 19, all other viral tested for and ruled out. The pt just returned from socializing in NYC without observing precautions.