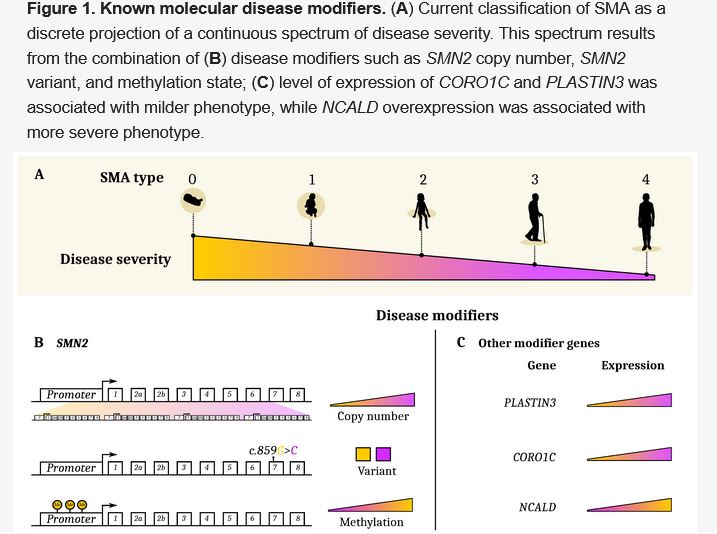
Known molecular disease modifiers. (A) Current classification of SMA as a discrete projection of a continuous spectrum of disease severity. This spectrum results from the combination of (B) disease modifiers such as SMN2 copy number, SMN2 variant, and methylation state; (C) level of expression of CORO1C and PLASTIN3 was associated with milder phenotype, while NCALD over expression was associated with more severe phenotype.
STANFORD, CA — While much of the research on spinal muscular atrophy has focused on children, adults make up more than one-third of all SMA cases.
Most adults with SMA have type 3, with symptoms that began in childhood or teens, but some have type 4 disease and may not have experienced any symptoms until their 30s. Because their presentations can vary substantially, sometimes a person with type 3 or 4 SMA may join the service before symptoms appear.
These individuals may receive care through the VA, particularly as progressive spinal muscular atrophy is considered a presumptive service-connected disability as an organic disease of the nervous system if it develops during active duty or within the applicable time limit.
The VA’s multidisciplinary patient aligned care teams (PACTs) are particularly well suited to providing care for patients with SMA as adult patients are likely to experience multiple organ system involvement, requiring the coordination of multiple specialists. Optimal management of SMA requires integrated acute care, physical therapy, cardiology, neurology, pulmonology, gastroenterology, orthopedics, nutrition and pharmacy.
Pharmacological Approach
Adult patients with SMA might benefit from drugs that increase the production of full-length SMN protein. The first clinical trial of an SMN-enhancing drug in adults, found that the oral agent risdiplam stabilized disease progression in 57.1% of young adult patients vs. 37.5% for participants receiving placebo. Anecdotally, adult patients have also reported recovering the ability to move to a upright sitting position using only core muscles. The level of SMN protein increased four-fold and was detectable in tissues throughout the body, which may help with some of the non-motor complications of SMA. The intrathecally injected nusinersen is also approved for use in adults.
Patients also could benefit from combining one of the SMN-enhancers with treatments that act on other affected parts of the body, particularly muscles. One drug in development blocks the production of myostatin, a molecule that inhibits muscle growth. Another slows the release of calcium from the regulatory troponin complex, which may increase the ability of muscles to contract. A clinical trial of the second investigational agent demonstrated an increased aerobic capacity and endurance as well and improved maximal expiratory pressure. Increasing function by protecting and building muscle may be especially useful for older SMA patients with milder forms of the disease.
Non-pharmacological considerations
The provider team can provide ongoing support to patients with SMA by working together to ensure healthy habits and appropriate non-pharmacological interventions.
While many patients with neuromuscular disorders have historically been advised to refrain from exercise to avoid muscle injury, current evidence supports regular activity to maintain flexibility and strength. Swimming or water exercise, weight-bearing aerobic activities, yoga, and resistance therapy have been found to be useful in moderation, according to recommendations from Tina Duong, MPT, PhDc, of Stanford University School of Medicine, and Bakri Elsheikh, MD, of The Ohio University Wexner Medical Center in Columbus, OH, who recommend about a half an hour of exercise two to five times a week.
They caution to “watch for fatigue and overuse weakness from overwork” with aerobic exercise, which can lead to decreased intensity. They also advise incorporating exercise into daily activities. While strengthening and aerobic exercise are not shown to improve strength, they do improve aerobic capacity and have no deleterious effects.
In addition, regular exercise helps patients maintain an optimal weight, an important consideration in individuals with reduced mobility. Excess weight can strain joints, increase pressure on the back, and further reduce movement. Overweight may also increase the risk of cardiovascular disease and sleep apnea.
Sleep-disordered breathing occurs in 40% and obstructive sleep apnea affects nearly one-quarter of individuals with neuromuscular disease. As the symptoms of sleep apnea may be mistaken for progression of SMA, physicians at the James H. Quillen VA Healthcare System in Mountain Home, TN, encouraged providers to “be watchful for reversible conditions that are associated with or are a complication of their primary disorder.” They noted that “early diagnosis and therapy directed toward these treatable disorders can contribute to an improved quality of life and may lengthen patient survival.”2
The International Standard of Care Committee for SMA recommends physical therapy for patients with SMA. Physical therapy can preserve walking ability, prevent joint contractures, and strengthen muscles. Physical therapists may also recommend mobility aids, orthotics, and assistive devices.
Many patients with SMA suffer from some degree of scoliosis and many will require ultimately require back surgery to ensure that the spinal curvature does not threaten proper respiratory function. Surgeons, pulmonologists, and neurologists will need to work together with physical therapists to achieve the best outcomes.
Women with SMA planning or managing a pregnancy may also need the support of high-risk obstetricians working in tandem with a neurologist and a pulmonologist familiar with SMA. Elsheikh and colleagues found that nearly three-quarters of women reported increased weakness during pregnancy that continued into the post-partum period for 42% of the mothers.1
Struggling with SMA day-in and day-out and concerns about losing mobility or independence increases the risk of depression and anxiety. Primary care providers may recommend a mental health specialist to help patients work through emotions associated with SMA, identify coping mechanisms, and select other treatment options. Some patients find that connecting with other adults with SMA through online groups or local organizations that meet in person can mitigate feelings of isolation and facilitate sharing of management techniques.
- Elsheikh BH, Zhang X, Swoboda KJ, et al. Pregnancy and delivery in women with spinal muscular atrophy. Int J Neurosci. 2017; 127(11): 953–957.
- Puruckherr M, Mehta JB, Girish MR, Byrd RP Jr, Roy TM. Severe obstructive sleep apnea in a patient with spinal muscle atrophy. Chest. 2004 Nov;126(5):1705-7. doi: 10.1378/chest.126.5.1705. PMID: 15539750.