Click To Enlarge
ATLANTA — As the nation’s largest healthcare system, the VA treats more individuals with hematological malignancies than any other organization in the United States. Beyond sheer numbers of patients, the VA has a special interest in blood cancers driven by two unique factors in the veteran population: increased risk from exposure while serving in the military and elevated risk based on age.
Exposure to high-energy radiation and certain chemicals, including Agent Orange, aqueous film-forming foam and asbestos, increased the risk of blood cancers in some veterans. For most veterans, however, simply aging puts them at elevated risk of these diseases.
More than half of individuals diagnosed with non-Hodgkin lymphoma are older than 65, with age-specific incidence rates ticking up steadily from the mid-40s to mid-50s and then rising sharply in the late 50s. Most leukemias follow a similar pattern, with a median age at diagnosis for acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL) or chronic myeloid leukemia (CML) all above age 65. The age correlation is clearer still in multiple myeloma (MM), just over one-third of patients with MM are under age 65. The median age of male veterans is 65, putting them squarely in the higher-risk zone for these diseases.
For the VA and veterans it serves, the 63rd American Society of Hematology (ASH) Annual Meeting in December in Atlanta brought some good news in terms of treatments and outcomes for blood cancers. A number of presentations specifically focused on elderly populations, including those age 80 and older, who are often excluded from clinical trials.
Improved Transplantation
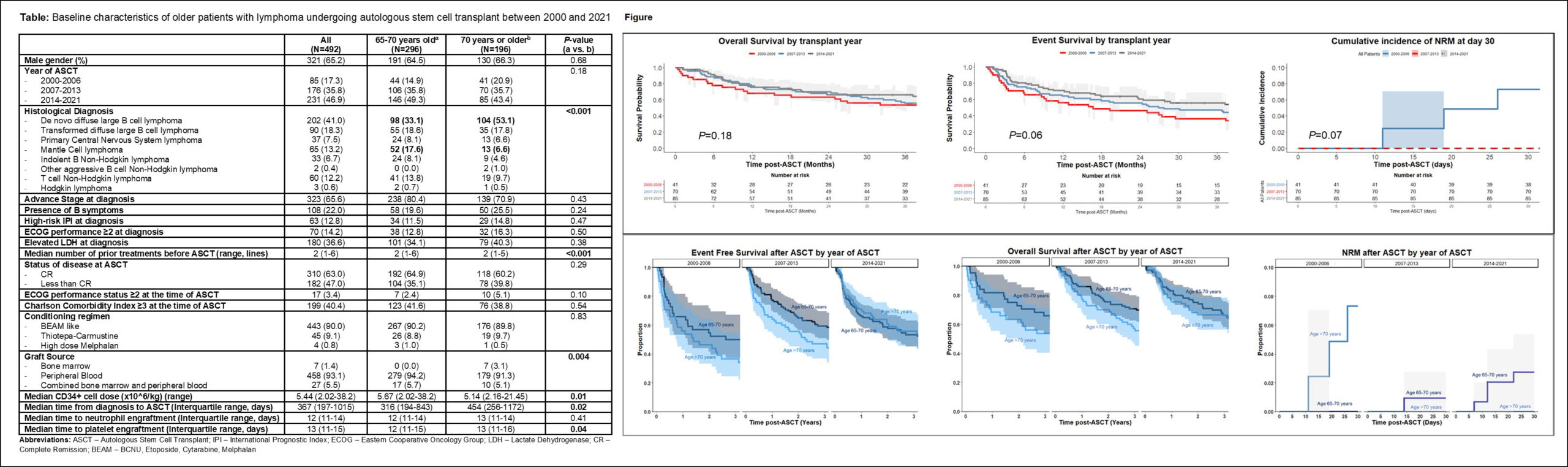
Perhaps the best news came from a study of autologous transplantation in patients older than 70 years. In a presentation by Kitsada Wudhikarn, MD, researchers at the Mayo Clinic in Rochester, MN, presented results of a study that included all patients diagnosed with lymphoma who underwent autologous stem cell transplant (ASCT) between January 2000 and February 2021 at their clinic. ASCT has long been the preferred treatment for patients with high-risk or relapsed lymphoma, but older patients are often denied the option for ASCT because of concerns about their ability to withstand it and earlier studies that showed poorer outcomes for older patients.1
The Mayo Clinic’s study included 196 patients with lymphoma who were age 70 or older. Of those, 24 patients were older than 75 and 76 had a Charlson comorbidity index of 3 or greater. The researchers compared this group to patients aged 65 to 70. The most common reason for transplant was relapsed diffuse large B-cell lymphoma.
More than 90% of the older patients received a peripheral blood graft with a median CD34+ cell dose of 5.14×106 cells/kg, significantly lower than that received by younger patients (P=0.01). Among the patients over age 70, the 30-day and 100-day nonrelapse mortality (NRM) were 1.5% 1.5% (95%CI 0-3.2%) and 4.6% (95%CI 1.6-7.5%), respectively, with little difference between those 70 to 75 and patients aged 75 and older.
At a median follow-up of 48 months, two-year event-free survival (EFS) was 55.9% (95%CI 49.2-63.5%) and overall survival (OS) was 67.4% (95%CI 61.0-74.5%) for the entire group. While the 70+ group had similar event-free survival to those age 65 to 70, the overall survival rate was lower. No difference in EFS or OS was detected between those 70 to 75 and those 75 and older. The 30-day nonrelapse mortality, two-year event-free survival and two-year overall survival all improved over the time period studied.
“Outcomes of ASCT in older patients with lymphoma have improved over time with an excellent 30-day NRM (0%) in the past recent years,” the team concluded. “The major cause of treatment failure after ASCT was progressive disease. With appropriate patient selection, ASCT in older patients is feasible and provides acceptable outcomes comparable to the patients from younger age group.”
Two other studies may change the care of treatment-naïve patients with CLL. The phase 3 trial A041202 demonstrated superior progression-free survival for older patients who receive the Bruton’s tyrosine kinase (BTK) inhibitor ibrutinib compared to those who received bendamustine plus rituximab (BR).2
“This update of the A041202 trial continues to show that ibrutinib regimens prolong [progression-free survival] over BR for older patients with treatment-naïve CLL. With longer follow-up, these benefits continue to be seen across subgroups, including those associated with higher risk disease,” the researchers noted. “Strikingly, within the ibrutinib arms, there does not appear to be inferior PFS for patients with abnormalities in TP53, the highest risk feature seen in CLL, and a predictor of inferior PFS with ibrutinib in relapsed CLL. This differentiates ibrutinib (and perhaps BTKi in general) from other targeted therapy paradigms for treatment-naïve CLL.”
The study continued to show low rates of complete response and the consequent need for continuous therapy, however, which lead to higher rates of toxicity. That prompted the researchers to launch a second study. To reduce the exposure to ibrutinib, researchers led by Jennifer Woyach, MD, at the Ohio State University in Columbus, Ohio, are comparing the effects of adding obinutuzumab and venetoclax to ibrutinib compared to adding only obinutuzumab. Ventoclax has shown an ability to produce complete response and minimal residual disease negative response in patients with untreated CLL with and without obinutuzumab.3
The study is enrolling patients with CLL or SLL who are age 70 or older and have not previously received treatment. “Results of this study have the potential to change the standard of care for older patients with previously untreated CLL,” the researchers said.
- Wudhikarn K, johnson BK, Willasboas JC. Improvement in Outcomes of Autologous Stem Cell Transplant in Patients with Lymphoma Older Than 70 Years: The Significance of Age in 2020s Abstract 2908. ASH 2021. Dec. 12, 2021.
- Wayach JA, Ruppert AS, Heerema NA. Long-Term Results of Alliance A041202 Show Continued Advantage of Ibrutinib-Based Regimens Compared with Bendamustine Plus Rituximab (BR) Chemoimmunotherapy. Abstract 639. ASH 2021. Dec. 13, 2021.
- Wayach JA, Ruppert AS, Perez G. A041702: A Randomized Phase III Study of Ibrutinib Plus Obinutuzumab Versus Ibrutinib Plus Venetoclax and Obinutuzumab in Untreated Older Patients (≥ 70 Years of Age) with Chronic Lymphocytic Leukemia (CLL). Abstract 3728. ASH 2021. Dec. 13, 2021.