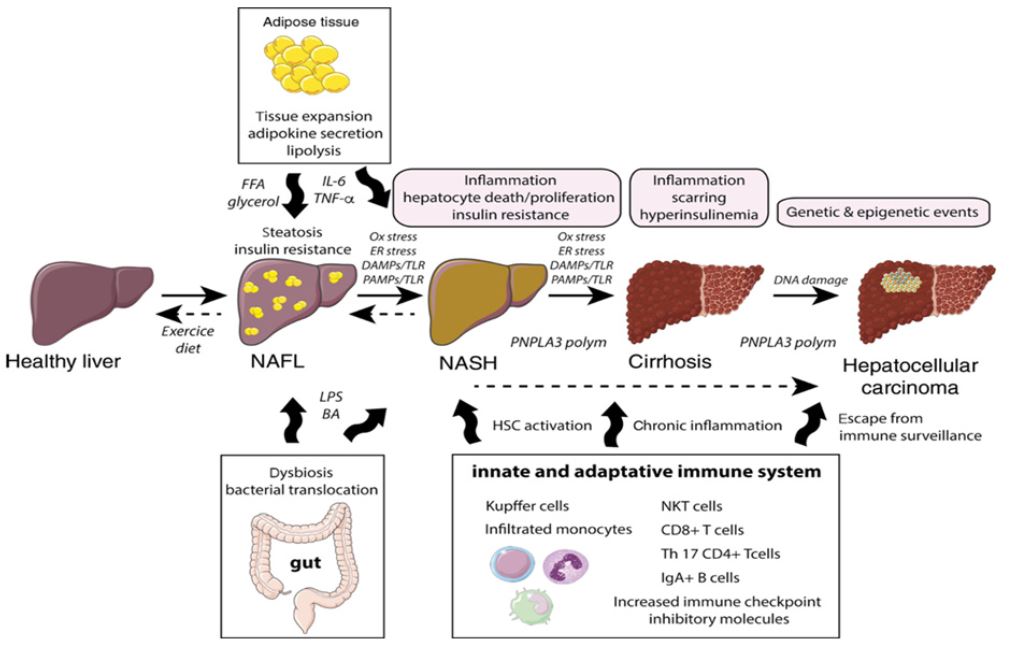
Click To Enlarge: Diagram of the pathophysiology of NAFLD-related hepatocellular carcinoma. NAFLD, non-alcoholic fatty liver disease. Figure reproduced with permission from DeGruyer publishing. The figure is from Lequoy M, Gigante E, Couty JP, Desbois-Mouthon C. Hepatocellular carcinoma in the context of non- alcoholic steatohepatitis (NASH): recent advances in the pathogenic mechanisms. Horm Mol Biol Clin Investig. 2020 Feb 29;41(1):/j/hmbci.2020.41.issue-1/ hmbci-2019-0044/hmbci-2019-0044.xml. doi: 10.1515/hmbci-2019-0044. PMID: 32112699
HOUSTON — What factors are behind delays in diagnosis of hepatocellular carcinoma in veterans who have cirrhosis of the liver?
A recent study examined the frequency of delayed diagnosis and the factors involved in a cohort of VHA cirrhosis patients. Results were published in Clinical Gastroenterology and Hepatology.1
For the retrospective study, Michael E. DeBakey VAMC researchers collected and analyzed data from the VHA’s electronic health records. They focused on factors associated with a delay in diagnosis of HCC of more than 60 days following a “red flag,” which was defined as the earliest date at which a diagnosis of HCC could have been made, based on American Association for the Study of Liver Disease 2005 guidelines.
The study team also looked at the effects of delayed diagnosis on survival, adjusting for patient and provider characteristics.
Results indicated that, among 655 patients with cirrhosis and a diagnosis of HCC from 2006 through 2011, 46.9% had a delay in diagnosis of more than 60 days following a red flag for HCC.
Researchers reported that delays in diagnosis for more than 60 days were significantly associated with:
- lack of provider adherence to the guidelines (adjusted odds ratio [OR], 4.82; 95% CI, 3.12-7.45),
- a diagnostic imaging evaluation instead of only the measurement of alfa fetoprotein (adjusted OR, 2.63; 95% CI, 1.09-6.24), and
- diagnosis as an incidental finding during examination for an unrelated medical problem (compared with an HCC-related assessment) (adjusted OR, 2.26; 95% CI, 1.09-4.67).
“This may be in part due to confusion among providers about which practice guideline to follow, as well as the complexity of HCC diagnostic imaging criteria and radiology reporting,” the authors wrote, recommending more standardized training for clinicians, more multidisciplinary care for patients at high risk for HCC and greater use of HCC tumor boards in the diagnostic process.
Surprisingly, the study also found that diagnostic delays of 60 days or more were associated with lower mortality compared to patients without a delay in diagnosis (unadjusted hazard ratio, 0.57; 95% CI, 0.47-0.68 and adjusted hazard ratio, 0.63; 95% CI, 0.50-0.78). “One possible explanation is that patients who presented with more advanced or worse cirrhosis severity may have received more urgent follow-up than patients with small, slow growing tumors and compensated cirrhosis,” according to the authors, who advised more research on that issue.
“Nearly half of veterans with cirrhosis have delays in diagnosis of HCC of 60 days or more after a red flag, defined by guidelines,” the authors wrote. “Interventions are needed to improve timely follow-up of red flags for HCC and adherence to guidelines, to increase early detection of HCC.”
The issue is not limited to veterans, however. An article written by authors from Inova Fairfax Medical Campus, in Falls Church, VA, pointed out that the prevalence of hepatocellular carcinoma (HCC) is increasing worldwide, while that measurement is decreasing for most other cancers.
“Non-alcoholic fatty liver disease (NAFLD), which has increased with the epidemics of obesity and Type 2 diabetes, increases the risk of HCC. Interestingly, NAFLD-associated HCC can develop in patients with or without cirrhosis,” according to the article in JHEP Reports. “A lack of awareness about NAFLD-related HCC has led to delays in diagnosis.”2
As a consequence, many patients with HCC are diagnosed with advanced-stage HCC, with reduced five-year survival.
To help avoid that issue, the study listed the following key points to consider:
- • NAFLD/NASH liver diseases are becoming the leading cause for HCC.
- • NAFLD-related HCC can develop in those with and without cirrhosis.
- • The presence of Type 2 diabetes increases the risk of HCC 2-fold and risk of death from HCC 1.5-fold.
- • The presence of metabolic syndrome along with Type 2 diabetes increases the risk of HCC 5-fold.
- • Obesity (BMI >30 kg/m2) doubles the risk of HCC, while a BMI >35 kg/m2 quadruples the risk of HCC.
- • Nonobese persons with metabolic comorbidities are at risk of NAFLD and NAFLD-related HCC.
- • Waist circumference as a surrogate for visceral obesity is an important measure to consider in addition to BMI when assessing risk of HCC.
- • NAFLD-related HCC tumors are large and can be hypervascular.
The review pointed out the low level of disease awareness about NAFLD and NAFLD-related HCC “which leads to diagnostic delays and contributes to late-stage diagnosis of HCC with high mortality. Continued education of health care providers and public health programs about NAFLD, its risk factors, associated outcomes (including HCC), diagnosis, and preventative measures are urgently needed.”
- Choi DT, Davila JA, Sansgiry S, David E, Singh H, El-Serag HB, Hsiao-Fan Sada Y. Factors Associated With Delay of Diagnosis of Hepatocellular Carcinoma in Patients With Cirrhosis. Clin Gastroenterol Hepatol. 2021 Aug;19(8):1679-1687. doi: 10.1016/j.cgh.2020.07.026. Epub 2020 Jul 18. PMID: 32693047; PMCID: PMC7855025.
- Younossi ZM, Henry L. Epidemiology of non-alcoholic fatty liver disease and hepatocellular carcinoma. JHEP Rep. 2021 May 11;3(4):100305. doi: 10.1016/j.jhepr.2021.100305. PMID: 34189448; PMCID: PMC8215299.
