Click to Enlarge: Personalized Multilevel Intervention for Improving Appropriate Use of Colorectal Cancer (CRC) Screening in Older Adults Source: JAMA Network
ANN ARBOR, MI — Each year, the VA diagnoses some 4,000 new cases of colorectal cancer (CRC) in veterans. Colorectal cancer screening can help detect cancer early, when it is most treatable. But the benefits of screening in older adults varies by individual, according to a new study.
Recently, Sameer D. Saini, MD, MS, led the new study to understand the effect of a personalized multilevel intervention on screening orders in older adults due to average-risk CRC screening.
“In older adults, the benefit of colorectal cancer screening, and indeed all preventive services, varies for each individual according to a multitude of factors,” said Saini, professor of gastroenterology at the University of Michigan and director of the VA Ann Arbor, MI, HSR&D Center for Clinical Management Research (CCMR), a VA HSR&D Center of Innovation. “These can be boiled down to two key elements: risk of cancer and life expectancy.”
Both these vary over a continuum—that is, they do not change abruptly at a given age— of and doctors can’t estimate either with certainty, Saini said. Data suggest that this complexity can get lost in a busy clinic visit. For example, screening rates drop abruptly after age 75, regardless of overall health.
“We wanted to test a more systematic, nuanced, personalized approach in older adults due for average risk colorectal cancer screening, one that took into account individual benefit and harm as well as personal values and preferences,” Saini explained.
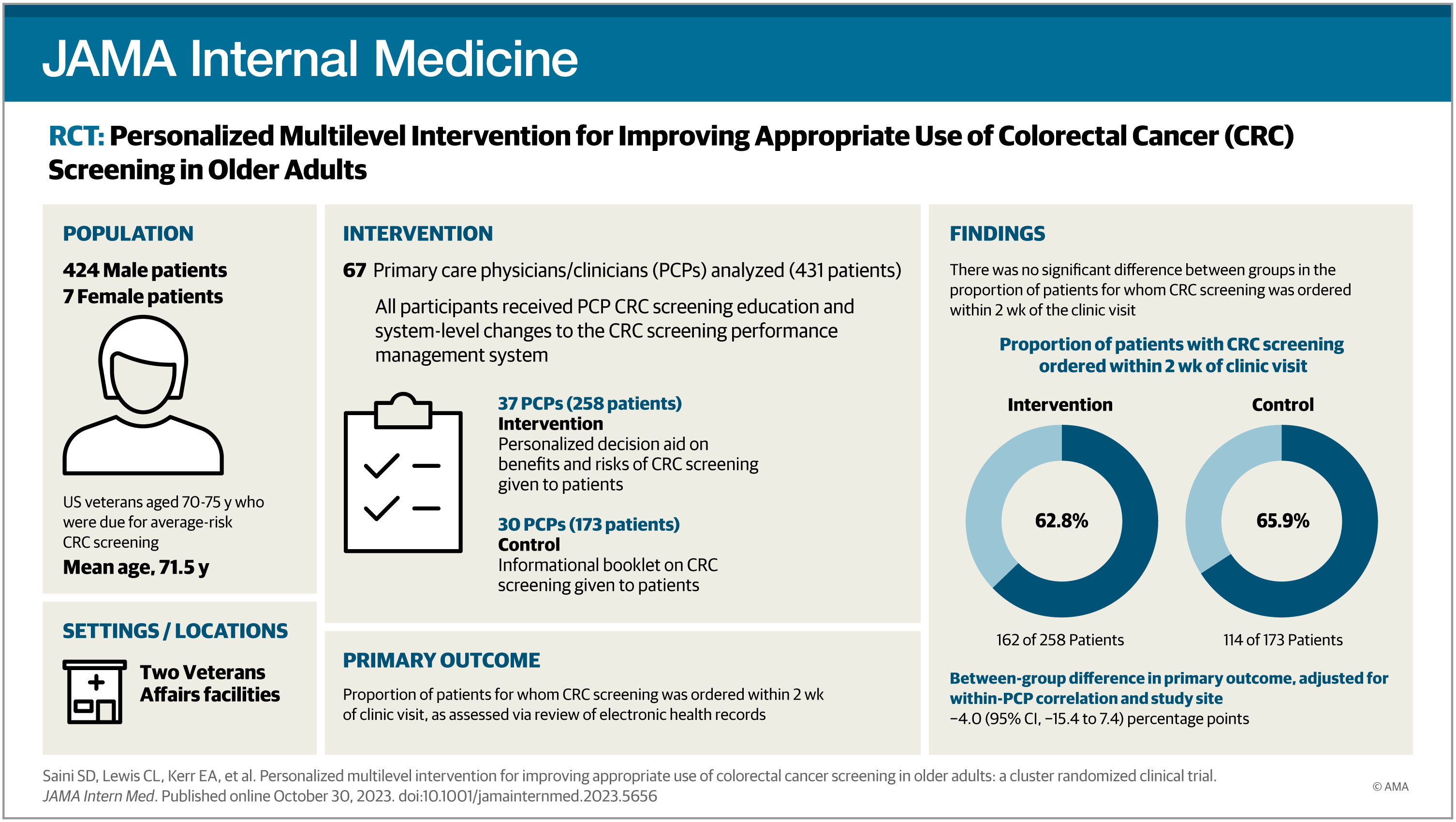
To test this personalized approach, Saini and his colleagues conducted a cluster randomized controlled trial from November 2015 to February 2019 at two sites within the VA health system—one academic VAMC and one of its connected outpatient clinics. The population was 431 average-risk veterans aged 70-75 who were attending a primary care visit and due for colorectal screening.1
Results were published recently in JAMA Internal Medicine.
The researchers began by developing a multilevel intervention designed to align screening use with screening benefit. The intervention had three key components: a personalized decision-aid booklet for patients; education of clinicians about screening benefits and harms for individual patients; and modifications to the CRC screening performance management system to support personalized screening decisions.
Clinicians and patients were randomized into an intervention and control arm. The intervention group received a multilevel personalized intervention, including a decision-aid booklet with detailed information on screening benefits and harms, personalized for each participant based on age, sex, prior screening and comorbidity. The control group received a simple educational booklet.
Participants received the booklet immediately before their primary care visit. The researchers then measured screening orders two weeks after the visit.
The researchers said their findings revealed that “older screen-due adults who were presented with detailed, personalized information about screening benefits and harms immediately before a primary care visit were more likely to receive screening orders concordant with benefit and were subsequently less likely to utilize screening overall than those who were not.”
“That is, individuals with low benefit from screening had a reduction in screening orders, and individuals with high benefit had an increase in screening orders,” Saini said. “Overall, this balanced out, resulting in no overall change in screening orders across the entire intervention arm compared to the control arm.”
Saini said the study was possible due to the integration of the VA system. “Our intervention was multilevel—it required engagement of not only patients, but also clinicians and the health system to align education and reminders,” he said. “This is not easy to do in a healthcare system that is not integrated like the VA.
Moreover, VA has always been a leader in undertaking innovative research in this space, where complex data and patient engagement methods are used.”
He said the study’s findings have several important implications. “First, it suggests that we can personalize screening in older adults by sharing detailed information with them. Second, it suggests that we can do so without substantially increasing clinician time. Third, similar approaches could be tested in other preventive services,” he said.
“We continue to develop strategies to scale the approach described in this study by partnering with health systems and other groups so that clinicians and patients can personalize screening in a pragmatic way as appropriate.”
- Saini SD, Lewis CL, Kerr EA, Zikmund-Fisher BJ, et al. Personalized Multilevel Intervention for Improving Appropriate Use of Colorectal Cancer Screening in Older Adults: A Cluster Randomized Clinical Trial. JAMA Intern Med. 2023 Oct 30:e235656. doi: 10.1001/jamainternmed.2023.5656. Epub ahead of print. PMID: 37902744; PMCID: PMC10616770.
