SEATTLE — According to a report from the national Centers for Disease Control and Prevention, more than 42,000 Americans died from an opioid overdose in 2016—five times higher than only seven years prior—and current CDC data shows little evidence that those numbers are any lower for 2017.
At the same time, according to the National Institute on Drug Abuse, opioids account for the greatest proportion of prescription drug abuse and mortality and that increasing addiction rates are directly related to increases in prescribing and easy availability of the drugs.
Veterans have proven to be disproportionately affected and are twice as likely to die from accidental overdoses of opioids as the general population.
For years, VA’s reputation when it came to opioids—deserved or not—was for overprescribing the highly addictive drugs, both in terms of dosage per patient and in numbers of prescriptions nationwide. Now VA seeks to be on the forefront of the fight against the epidemic, taking the lead in cutting the number of prescriptions, creating transparency in prescribing practices and by promoting medication-assisted opioid addiction treatment.
In 2013, a report by the Center for Investigative Reporting sent off shock-waves in Congress and the veteran community when it showed that VA prescriptions of hydrocodone, oxycodone, methadone and morphine increased by 270% in the 12 years prior. The report triggered congressional hearings where VA physicians at some facilities testified that they felt pressured to prescribe the powerful painkillers, while receiving inadequate training in pain management.
While the increase in opioid prescribing was not limited to VA—sales of prescription opioids in the U.S. nearly quadrupled from 1999 to 2014, according to the CDC—VA found itself in the spotlight and searching for ways to curb a dangerous trend.
That same year, VA began implementing its Opioid Safety Initiative (OSI). Designed to help decrease opioid prescribing practices associated with adverse outcomes, key components of OSI included the creation of a dashboard tool that tracks electronic medical data to audit opioid-related prescribing in real-time. The dashboard not only tracks opioid prescriptions but also focuses on high-dose opioid prescriptions and concurrent opioids and benzodiazepine prescriptions—a combination seen in patients suffering from PTSD. That combination, as well as high-dose prescriptions, increased the chances of deadly overdoses.
The OSI also identifies a clinical leader at each facility whose role is to implement the tool and promote safer prescribing; coordinating pain management to include patient and provider education, testing and tapering programs, and non-opioid pain management therapies.
The OSI has been credited with a sharp decrease in opioid prescribing in VA during the five years following its implementation. In 2017, 471,000 veterans received opioid prescriptions through VA, down from a peak of about 679,000 in 2012.
According to a VA report prepared last year, the OSI has not only resulted in fewer patients getting opioids but in fewer patients on concomitant benzodiazepines, fewer patients on high-dose opioids, more patients with informed consent and drug screenings, and a near universal pain management education of prescribers.
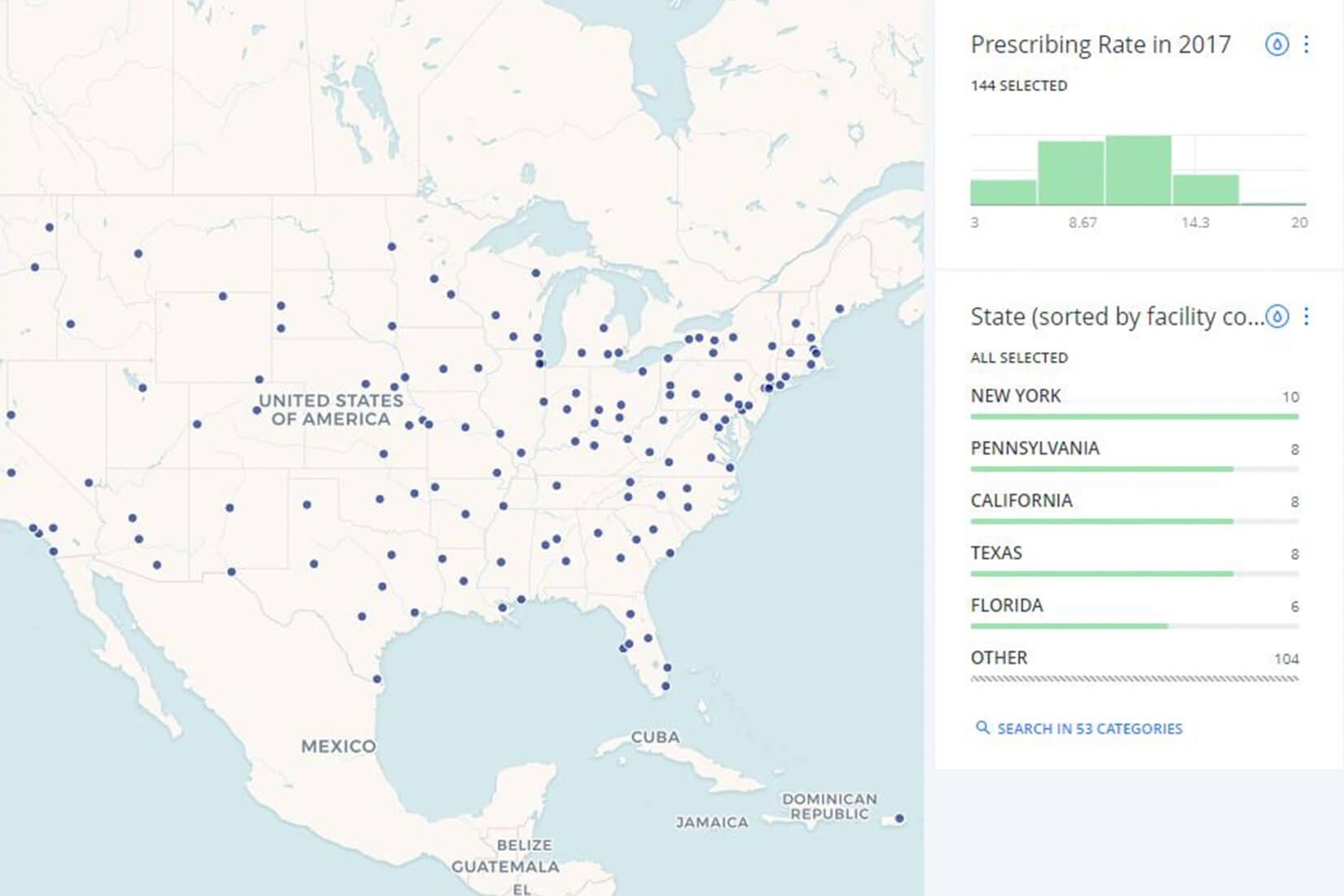
In January, VA took the unprecedented step of posting its opioid-prescribing rates for each facility online. The interactive map tracks each VA medical center and lists its current prescribing rate by percentage of patients, its rate in 2012 and the percentage that number has increased or decreased. According to VA, 99% of facilities have decreased prescribing rates since 2012. The agency intends to update the map semi-annually, in January and July of each year.
Addiction Treatment
While the number of opioid prescriptions dropped between 2012 and 2017, the number of veterans with an opioid-use disorder rose. Between 2010 and 2015, the number rose by 55%, reaching 68,000 in 2015. Research has shown that veterans of Iraq and Afghanistan are more susceptible than the general population, especially those patients diagnosed with PTSD.
But as the number of those addicted has risen, VA’s treatment efforts have grown proportionately. For over 30 years, VA has been at the forefront of substance abuse treatment and has led the way in medication-assisted opioid abuse treatment.
“In fact, we’re trying to move away from using the phrase ‘medication-assisted,’” explained Andrew Saxon, MD, director of the Center of Excellence in Substance Abuse Treatment and Education (CESATE) at the VA Puget Sound Health Care System. “Use the analogy of high blood pressure. If I start somebody on high blood pressure medication, we don’t call it medication-assisted treatment for HBP. It’s just treating high blood pressure.”
Just as medication is a common treatment option for HBP in conjunction with behavior modification, so should it be with opioid addiction, Saxon explained.
His experience with treating addiction with medication began in the mid-1980s. At the time, methadone was the go-to treatment program for opiate addicts and naltrexone—an opiate antagonist—had just been approved. Looking back now, Saxon is struck by how much has been learned and how much medication for addiction has improved—from better understanding of methadone dosing to the approval of injectable naltrexone and the development of buprenorphine.
“Buprenorphine is a partial agonist, so it has a great safety profile,” Saxon said. “And it has a ceiling effect on the respiratory depression effect. It’s virtually impossible for an adult to overdose on buprenorphine alone.”
These advancements have made medication therapy not only more effective but more convenient for providers. “The average provider can’t dispense methadone, but they can prescribe buprenorphine,” Saxon explained. “Advancements in medication treatment in the last 30 years have been extraordinary. We started with medication that people had to come into a clinic to get. Now we know so much more about that medication, and we have others that can be prescribed. If one medication doesn’t work, providers can try another.”
VA has been in a unique position to take the lead in the use of medication in opioid addiction therapy, Saxon explained. “Unlike the private healthcare sector, we are responsible for the lives of our patients for their whole lives. Many veterans come for our care when they separate from active duty and stay with VA for the duration of their lives.”
VA also has strong academic affiliations, with partnership programs between VAMCs and universities being common practice. “Academic medical centers tend to be on the forefront of treatment for most disorders,” Saxon said.
VA also had an infrastructure in place for other substance treatment programs, most commonly alcohol abuse. When opioid use became a significant problem, the department was able to branch off existing abuse programs to encompass opioid treatment, Saxon explained.
In FY 2017, about 36% of VA patients being treated for opioid use disorders were receiving medication treatment. That represents an increase of only 4.5% over the past 10 years. However, Saxon noted, the number of patients with such disorders doubled during that decade, which means that VA’s use of medication more than doubled during that time.
Nationally, medication use is not very common, Saxon noted. “Outside of VA, we believe that it’s a minority of opioid abuse patients that get any treatment. Many go to a 28-day abstinence-oriented inpatient program, or a short-term program where they can withdraw and get behavioral treatment. It’s shocking that, in our country as a whole, the rates of using the right treatment aren’t very good, with only 20% or so getting medication.”
VA is looking to improve its medication prescribing rates even more. The agency has begun focusing on lower-performing sites—those with fewer than 36% receiving medication—and working with those centers to lower barriers to patients getting treatment. VA also is looking to have a large train-the-trainer meeting focusing on opioids.
“The idea is to bring people nationally from around the country and train them on how to treat opioid use disorder in the outpatient setting. Then they’ll go back to their localities and become the champion for treatment there,” Saxon explained. “We’re doing way better than a lot of healthcare providers, but there’s still a long way to go.”