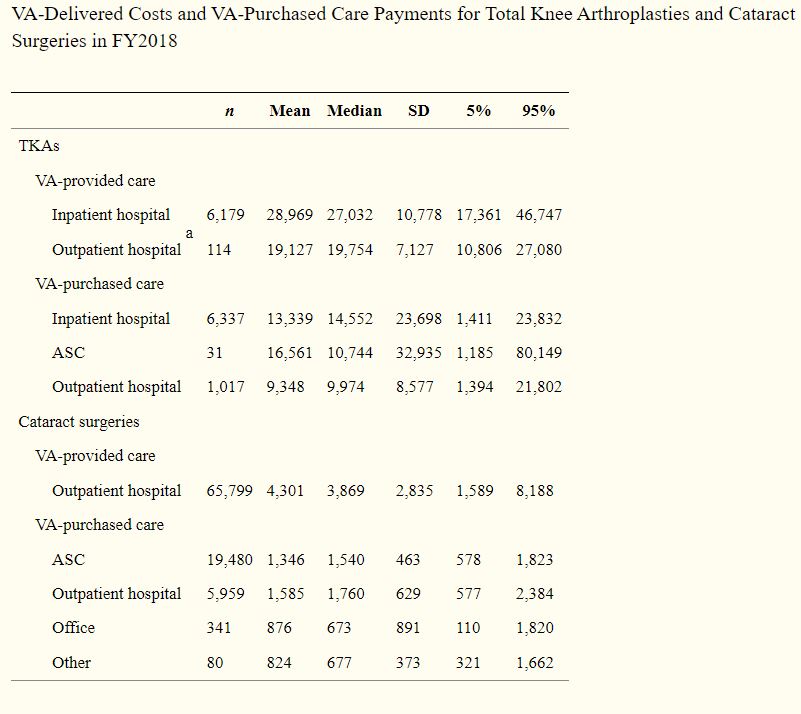
Click To Enlarge: SD, standard deviation; TKA, total knee arthroplasty; VA, Veterans Health Administration.
MENLO PARK, VA new study raises questions about which veterans requiring cataract and total knee replacement surgeries received community care, as opposed to the cases kept within the VA system.
The report in Medical Decision-Making Policy & Practice described how veterans’ access to VA-purchased community care expanded due to large increases in funding provided in the 2014 Veterans Choice Act.1
Researchers from three VA healthcare systems—Palo Alto in California, Boston and Salt Lake City—sought to compare costs between VA-delivered care and VA payments for purchased care for two commonly performed surgeries: total knee arthroplasties (TKAs) and cataract surgeries. Included were descriptive statistics and regressions examining costs in VA-delivered and VA-purchased care (fiscal year [FY] 2018 [October 2017 to September 2018]).
The bottom line was that VA costs for doing the procedures in-house were often higher than what they paid to community providers, although it wasn’t clear how much of that was due to the complexity of the patients or procedures.
The focus was on 13,718 TKAs, of which 6,293 (46%) were performed in VA, and 91,659 cataract surgeries, of which 65,799 (72%) were performed in VA. The study team looked at costs of VA-delivered care based on activity-based cost estimates, as well as costs of VA-purchased care based on approved and paid claims.
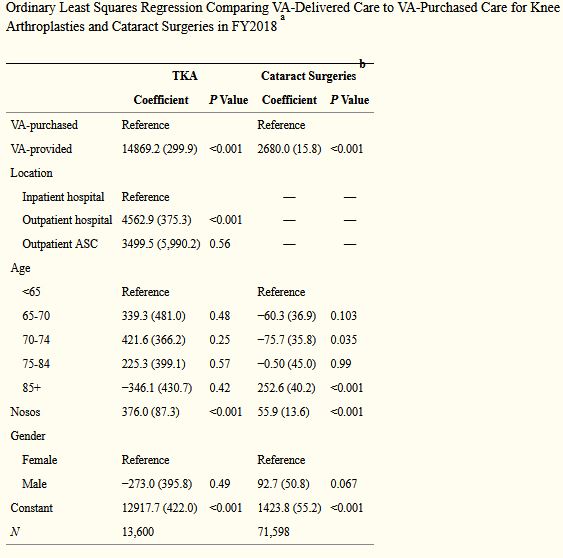
Click To Enlarge:
a. Standard errors (SE) adjust for clustering within person, in parentheses.
b. Estimated for outpatient only.
Results indicated that 98% of VA-delivered TKAs occurred in inpatient hospitals, with an average cost of $28,969 (SD $10,778). The majority (86%) of VA-purchased TKAs were also performed at inpatient hospitals, with an average payment of $13,339 (SD $23,698).
VA-delivered cataract surgeries, meanwhile, were performed at hospitals as outpatient procedures, with an average cost of $4,301 (SD $2,835). VA-purchased cataract surgeries performed at hospitals averaged $1,585 (SD $629), while those performed at ambulatory surgical centers cost an average of $1,346 (SD $463), according to the report.
“We also found significantly higher Nosos risk scores for patients who used VA-delivered versus VA-purchased care,” the researchers wrote.
“Costs of VA-delivered care were higher than payments for VA-purchased care, but this partly reflects legislative caps limiting VA payments to community providers to Medicare amounts,” the authors concluded. “Higher patient risk scores in the VA could indicate that community providers are reluctant to accept high-risk patients because of Medicare reimbursements, or that VA providers prefer to keep the more complex patients in VA.”
Higher Costs
Researchers point out that VA payments for cataract surgeries and TKAs in the community were less than the VA cost of providing these services in the VA, adding, “These differences offer opportunities for VA to examine why it has higher costs and, when appropriate, implement innovations to lower its costs. Through FY2018, VA conducted most of its cataract surgeries in operating rooms, which are encumbered with added fixed costs. Similarly, as of 2018, all VA-delivered TKAs were performed in the inpatient setting, whereas non-VA hospitals began to perform TKAs in ambulatory care with the passage of the CMS rule in January 2018 allowing reimbursement to hospital outpatient departments. Moving clinically appropriate procedures to less-intensive settings, some of which has already started, will be important for helping the VA to optimize its variable and fixed costs, possibly saving resources and expanding access in the long run.”
Background information in the article recounted how, in 2014, Congress enacted legislation to enable more veterans to receive VA-purchased care from community providers. Since then, however, little research has been done on costs and none on value of care, at least partly because the newness of VA’s claims database (PIT), according to the authors.
Still, they explained, “VA payments for cataract surgeries and TKAs in the community were less than the VA cost of providing these services in the VA. These differences offer opportunities for VA to examine why it has higher costs and, when appropriate, implement innovations to lower its costs. Through FY2018, VA conducted most of its cataract surgeries in operating rooms, which are encumbered with added fixed costs. Similarly, as of 2018, all VA-delivered TKAs were performed in the inpatient setting, whereas non-VA hospitals began to perform TKAs in ambulatory care with the passage of the CMS rule in January 2018 allowing reimbursement to hospital outpatient departments. Moving clinically appropriate procedures to less-intensive settings, some of which has already started, will be important for helping the VA to optimize its variable and fixed costs, possibly saving resources and expanding access in the long run.”
The article went on to elucidate how VA payments to community providers are based on the Choice and MISSION Acts, which cap VA payments using Medicare prices in most cases. Because VA payments were very similar to estimated Medicare payments published on CMS websites, possibly decreasing the need for future cost comparisons, VA can estimate its expected fee-for-service payments ahead of time, the researchers pointed out.
They suggested, “If community providers are concerned about VA’s reimbursement, the main options facing them include the following:
- not accepting VA cases,
- selecting patients based on risk,
- choosing a treatment or setting that maximizes reimbursement, or
- inducing demand for more services once a patient has been referred
Head-to-head comparisons may wish to examine these possible mechanisms directly.”
The study added, “Of these four options, our data highlight the need for more research on risk selection. We show that patients who received VA-purchased TKAs had half the risk score of patients receiving VA-delivered TKA. In prior work, we found considerable heterogeneity in veterans using community care, with lower risk scores for people enrolling in the Choice program compared to veterans who used the more traditional Fee program. Future work is critically needed to understand the differences in patient risk and whether this reflects patient selection, provider selection, or the “crowding-out” of services that were previously covered by Medicare.”
The authors emphasized that future research also should consider costs over time, “because the Choice and MISSION Act pay based on the Medicare fee schedule and do not place any constraints on quantity of services over time or value.”
- Wagner TH, Lo J, Beilstein-Wedel E, Vanneman ME, Shwartz M, Rosen AK. Estimating the Cost of Surgical Care Purchased in the Community by the Veterans Health Administration. MDM Policy Pract. 2021 Nov 16;6(2):23814683211057902. doi: 10.1177/23814683211057902. PMID: 34820527; PMCID: PMC8606928.