Findings in Patients Without Psychosis Offers Alternatives
Click to Enlarge: Source: The New England Journal of Medicine
BOSTON — Ketamine was found to be noninferior to electroconvulsive therapy (ECT) as therapy for treatment-resistant major depression without psychosis, according to a new study.
The report in the New England Journal of Medicine pointed out that ECT and subanesthetic intravenous ketamine are both currently used for treatment-resistant major depression, but, until now, the comparative effectiveness of the two treatments had remained uncertain.
Researchers from Mass General Brigham and Harvard Medical School and colleagues, including participation from the Michael E. DeBakey VAMC in Houston, conducted an open-label, randomized, noninferiority trial involving patients referred to ECT clinics for treatment-resistant major depression.
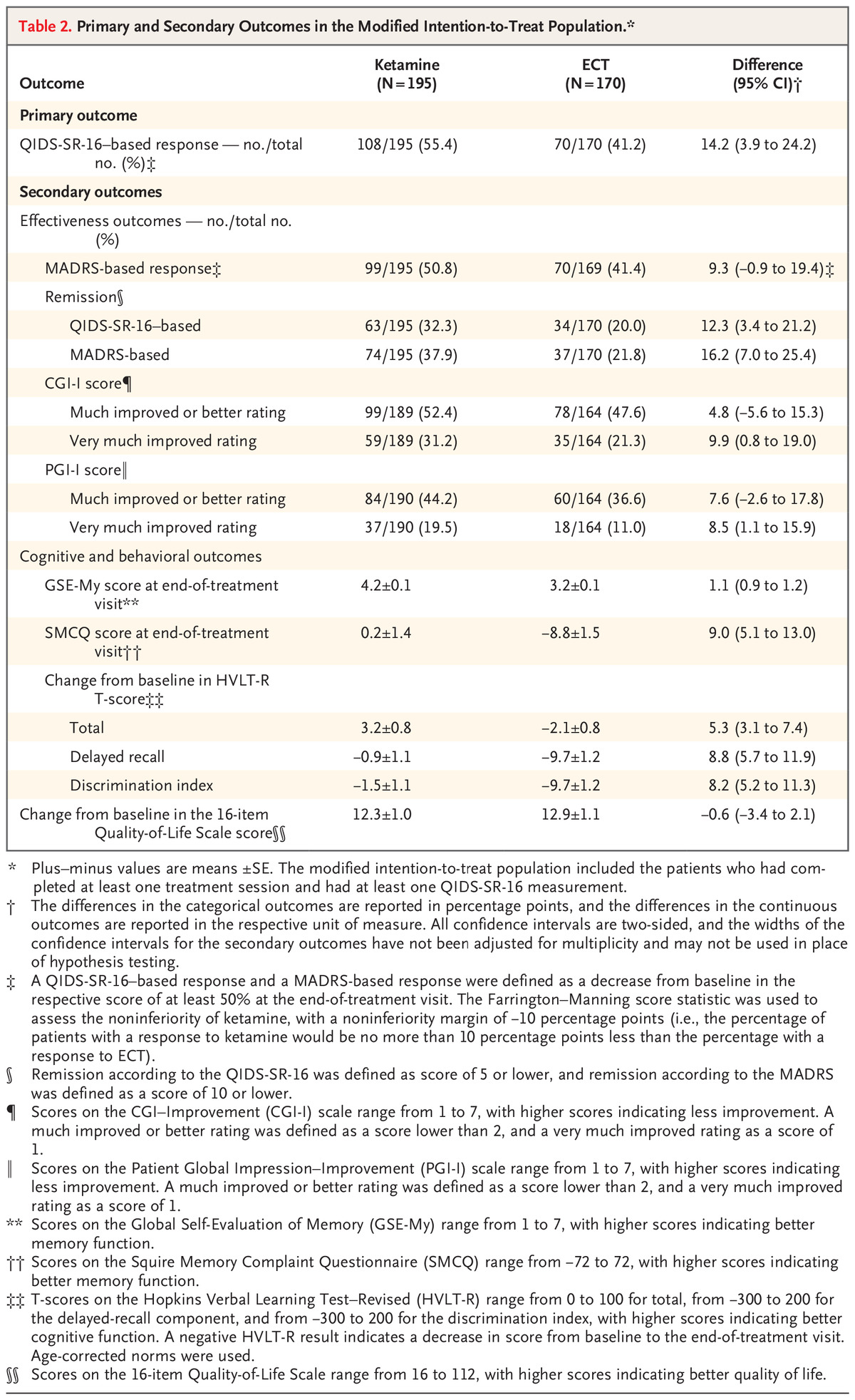
During an initial 3-week treatment phase,403 participants from five clinical sites either received ECT three times per week or ketamine (0.5 mg per kilogram of body weight over 40 minutes) twice per week. Designated as the primary outcome was a response to treatment; essentially a decrease of 50% or more from baseline in the score on the 16-item Quick Inventory of Depressive Symptomatology-Self-Report. (scores range from 0 to 27, with higher scores indicating greater depression). Scores on memory tests and patient-reported quality of life were considered secondary outcomes.
Following the initial treatment phase, responsive patients were followed over a 6-month period.
Results indicated that 55.4% of the patients in the ketamine group and 41.2% of those in the ECT group had a response (difference, 14.2 percentage points; 95% confidence interval, 3.9 to 24.2; P<0.001 for the noninferiority of ketamine to ECT).
The downside of ECT appeared to be a decrease in memory recall after three weeks of treatment (mean [±SE] decrease in the T-score for delayed recall on the Hopkins Verbal Learning Test-Revised, -0.9±1.1 in the ketamine group vs. -9.7±1.2 in the ECT group; scores range from -300 to 200, with higher scores indicating better function), although gradual recovery occurred during follow-up.
“Improvement in patient-reported quality-of-life was similar in the two trial groups,” the authors wrote. “ECT was associated with musculoskeletal adverse effects, whereas ketamine was associated with dissociation.”
They pointed out, “Both ketamine and ECT appeared to be associated with improved quality of life immediately after the initial treatment phase.”
Antidepressants Suboptimal
The researchers concluded that ketamine was noninferior to ECT as therapy for treatment-resistant major depression without psychosis. Background information in the articles noted that major depressive disorder is a leading cause of disability worldwide and is estimated to affect 21 million adults in the United States.
“Although antidepressants are widely available, the effectiveness of antidepressants is suboptimal in more than [one-third] of patients,” according to the report. “Treatment-resistant major depression is commonly defined as depression with an unsatisfactory response to two or more adequate trials of antidepressants.”
The authors advised that ECT “has a track record of nearly 80 years as one of the most effective and rapid strategies for treatment-resistant major depression. Advancements in ECT, including administration while the patient is under brief general anesthesia, unilateral electrode placement, and refined techniques for seizure elicitation such as ultrabrief pulse stimulation, have enabled it to be more commonly performed as an outpatient procedure. However, ECT remains underused owing to limited availability, social stigma, and concerns regarding the adverse effect of cognitive impairment.”
Ketamine, meanwhile, is an N-methyl-d-aspartate receptor antagonist, that has been approved by the Food and Drug Administration as a sedative, analgesic and general anesthetic. “Over the past two decades, ketamine, administered intravenously at subanesthetic doses of 0.5 mg per kilogram of body weight, was noted to have a rapid antidepressant effect in patients with major depressive disorder and treatment-resistant major depression. Ketamine, in single or multiple doses, is increasingly being used for treatment-resistant major depression,” according to the report.
The authors called ketamine “an attractive alternative for patients because it does not require general anesthesia and is not associated with clinically significant memory impairment.” They cautioned, however, that “ketamine is a Schedule III medication with liability for potential abuse. Because treatment with ketamine can lead to transient changes in perception and thinking, it is mainly used in patients with treatment-resistant major depression without psychotic features.”
The researchers advised that their studies difference from some recent studies indicating that remission with ketamine was inferior to that with ECT. “Our trial differs from these reports in that it included only patients with major depressive disorder without psychosis (those with psychosis were excluded), had a larger sample size, and was performed in a primarily outpatient population (89% of patients),” they wrote.
The article also noted that, in the current trial, the percentages of patients who had a response or remission with ECT were lower than those in other reports.
“ECT has been shown to be more effective among older adults, among patients with major depressive disorder with psychosis, and in inpatient and research settings,” the authors wrote, adding that the results “of our pragmatic trial are more similar to the reports of lower rates of remission with ECT in community and outpatient settings than to reports of higher rates in inpatient and research settings.”
They went on to state that the current trend in the United States is for ECT to be administered on an outpatient basis to patients with treatment-resistant major depression. “ECT is recommended as being highly effective for rapid treatment of late-life, catatonic, and suicidal depression,” the researchers noted. “Future studies will need to be conducted to determine the comparative effectiveness of ketamine and ECT in older patients, patients with bipolar depression and in emergency inpatient settings.”
- Anand A, Mathew SJ, Sanacora G, Murrough JW, et. al. Ketamine versus ECT for Nonpsychotic Treatment-Resistant Major Depression. N Engl J Med. 2023 Jun 22;388(25):2315-2325. doi: 10.1056/NEJMoa2302399. Epub 2023 May 24. PMID: 37224232.