OAC Prescribing Low for Frail Veterans
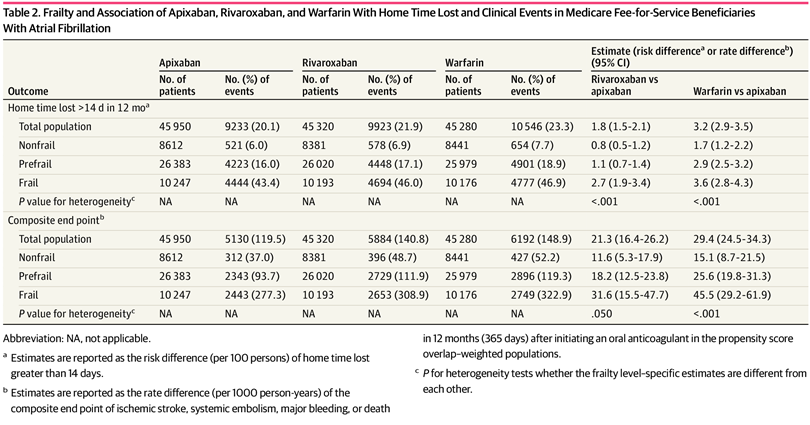
Click to Enlarge: Frailty and Association of Apixaban, Rivaroxaban, and Warfarin With Home Time Lost and Clinical Events in Medicare Fee-for-Service Beneficiaries With Atrial Fibrillation Source: JAMA Network Open
BOSTON — Past research has suggested that elderly veterans who are frail are less likely to be prescribed oral anticoagulants for atrial fibrillation (AF). A recent study suggested a possible way to mitigate some of those challenges.
The study, which looked at the association of frailty level with oral anticoagulant outcomes in patients with AF, concluded that apixaban might be preferred for older adults.
In the cohort study of 136,551 Medicare beneficiaries with AF, apixaban was associated with increased home time and fewer clinical events than rivaroxaban and warfarin, with greater differences among those with frailty. The researchers from Brigham and Women’s Hospital and Harvard Medical School also found that apixaban was associated with a lower cost than rivaroxaban but a higher cost than warfarin because of a higher anticoagulant cost.
The JAMA Network Open article pointed out the lack of data on patient-centered outcomes and healthcare costs by frailty in patients with AF who take OACs. That led the study team to compare home time, clinical events and healthcare costs associated with OACs by frailty levels in older adults with AF.1
The community-based cohort study assessed Medicare fee-for-service beneficiaries 65 years or older with AF from Jan. 1, 2013, to Dec. 31, 2019, with data analysis performed from January to December 2022.
The researchers used prescription claims to measure apixaban, rivaroxaban and warfarin use. Frailty was determined using a validated claims-based frailty index. Outcome measures were defined as:
- home time (days alive out of the hospital and skilled nursing facility) loss greater than 14 days;
- a composite endpoint of ischemic stroke, systemic embolism, major bleeding or death; and
- total cost per member per year after propensity score overlap weighting.
Included in the study were 136,551 beneficiaries, including 45,950 taking apixaban (mean [SD] age, 77.6 [7.3] years; 51.3% female), 45,320 taking rivaroxaban (mean [SD] age, 77.6 [7.3] years; 51.9% female), and 45,281 taking warfarin (mean [SD] age, 77.6 [7.3] years; 52.0% female).
Home Time Lost
“Compared with apixaban, rivaroxaban was associated with increased risk of home time lost greater than 14 days (risk difference per 100 persons, 1.8 [95% CI, 1.5-2.1]), composite endpoint (rate difference per 1000 person-years, 21.3 [95% CI, 16.4-26.2]), and total cost (mean difference, $890 [95% CI, $652-$1127]), with greater differences among the beneficiaries with frailty,” the authors advised. “Use of warfarin relative to apixaban was associated with increased home time lost (risk difference per 100 persons, 3.2 [95% CI, 2.9-3.5]) and composite endpoint (rate difference per 1,000 person-years, 29.4 [95% CI, 24.5-34.3]), with greater differences among the beneficiaries with frailty. Compared with apixaban, warfarin was associated with lower total cost (mean difference, -$1,166 [95% CI, −$1,396 to −$937]) but higher cost when excluding OAC cost (mean difference, $1,409 [95% CI, $1,177 to $1,642]) regardless of frailty levels.”
Background information in the study noted that the use of OACs remains suboptimal in older adults with AF. One of the main concerns is frailty, which complicates prescribing decisions, the authors suggest, because the condition is highly associated with the risk of bleeding, falls and drug-related adverse events.
They added, “Although the prevalence of frailty in older adults with AF ranges from 17% in the community to 62% in the hospital, patients with frailty are severely underrepresented in clinical trials, leading to limited data to inform OAC prescribing and suboptimal use in older adults with AF and with frailty. In a recent U.S. nationwide trend analysis, frailty was associated with 26% lower odds of OAC prescribing among older adults. However, the evidence generated based on routine care on OACs in patients with frailty remains limited, and no prior studies have investigated the use of OACs with a focus on patient-centered outcomes and health care costs among patients with AF and with frailty.”
A veteran study published last year in the Journal of General Internal Medicine agreed that frailty is often cited as a factor influencing OA prescription in patients with nonvalvular atrial fibrillation (NVAF). The Oregon Health & Science University-led study sought to determine the prevalence of frailty and its association with OAC prescription in older veterans with NVAF.2
Researchers from the New England GRECC at the VA Boston Health Care System and the Edith Nourse Rogers Memorial VA Medical Center in, Bedford, MA, were involved in the research.
The study team used ICD-9 codes in VA records and Medicare claims data to identify patients with NVAF and CHA2DS2VASC ≥2 receiving care between February 2010 and September 2015. Researchers examined rates of OAC prescription, further stratified by direct oral anticoagulant (DOAC) or vitamin K antagonist (VKA) use.
Participants were characterized into three categories: nonfrail, prefrail, and frail based on a validated 30-item EHR-derived frailty index.
Results indicated that, of 308,664 veterans with NVAF and a CHA2DS2VASC score ≥2, 121,839, (39%) were prescribed OAC (73% VKA). The mean age was 77.7 (9.6) years; CHA2DS2VASC and ATRIA scores were 4.6 (1.6) and 5.0 (2.9) respectively.
“Approximately a third (38%) were frail, another third (32%) were pre-frail, and the remainder were not frail,” the authors wrote. “Veterans prescribed OAC were younger, had higher bleeding risk, and were less likely to be frail than participants not receiving OAC (all p’s<0.001). After adjustment for factors associated with OAC use, pre-frail (OR: 0.89, 95% CI: 0.87-0.91) and frail (OR: 0.66, 95% CI: 0.64-0.68) veterans were significantly less likely to be prescribed OAC than non-frail veterans. Of those prescribed OAC, pre-frail (OR:1.27, 95% CI: 1.22-1.31) and frail (OR: 1.75, 95% CI: 1.67-1.83) veterans were significantly more likely than non-frail veterans to be prescribed a DOAC than a VKA.”
The study advised that high rates of frailty exist among older veterans with NVAF. “Frailty using an EHR-derived index is associated with decreased OAC prescription,” it concluded.
- Lin KJ, Singer DE, Ko D, et al. Frailty, Home Time, and Health Care Costs in Older Adults With Atrial Fibrillation Receiving Oral Anticoagulants. JAMA Netw Open. 2023;6(11):e2342264. doi:10.1001/jamanetworkopen.2023.42264
- Sanghai SR, Liu W, Wang W, Rongali S, et. al. Prevalence of Frailty and Associations with Oral Anticoagulant Prescribing in Atrial Fibrillation. J Gen Intern Med. 2022 Mar;37(4):730-736. doi: 10.1007/s11606-021-06834-1. Epub 2021 May 4. PMID: 33948795; PMCID: PMC8904680.
